2019: Volume 1, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFA Tale of Two Treatments
Ajay Mishra1, Sonia Mishra2, Jagdish P Mishra3
1Georgetown University 3700 O St NW, WA, USA 2MMS student at LECOM Erie, PA, USA 3Upstate Cardiology, 215 Summit St. Batavia, NY, USA
*Corresponding author: Jagdish P Mishra* Upstate Cardiology, 215 Summit St. Batavia, NY 14020, USA.
Received: November 9, 2019 Published: November 27, 2019
Keywords: Coronary Artery Disease (CAD), Myocardial Infarction (MI), Stenting, Angina
INTRODUCTION
There are about 9 million people in the US diagnosed with angina and there are close to 500,000 cases diagnosed with chest pain/angina every year [1]. Probably 50% of the patients that I see everyday in my practice have either history of chest pains, diagnosed with coronary artery disease (CAD), have had a myocardial infarction (MI) or have undergone stenting or cardiac bypass surgery.
Lately I encountered two patients in my office within one month with chest pains, one with underlying CAD and the other having a myocardial infarction (MI). I sent them to one hospital for further management and both came out with what I call less-than optimal treatment strategy. Therefore they were sent back to another hospital and the treatment recommended was different in each case with optimal symptom relief and complete patient satisfaction.
Let me explain:
PATIENT #1
A 56-year old man with a history of hypertension and possible controlled GERD symptoms was seen in my office for chest pains starting for about a month before his visit. His symptoms of chest pressure and chest pains were exertional in nature and relieved by rest, mostly centrally located in the chest and not associated with any dizziness, diaphoresis or palpitations. There was no history of jaw or arm pains. He was quite apprehensive, concerned and anxious about these symptoms. He did not smoke tobacco and there was no family history of premature coronary artery disease, heart attacks or strokes.
He walked on the treadmill in my office for 4.40 minutes and developed similar chest tightness/chest pains. At his request, the treadmill was stopped. His baseline EKG was normal and his treadmill stress test did not show any ischemic ST/T changes (at 4.40 minutes of exercise, and 7 METS of workload).
He was started on Metoprolol succinate 25 mg a day, aspirin with food 81 mg a day and Rosuvastatin 10 mg a day. His initial symptoms and reproduced symptoms were quite suggestive of angina related to ischemic heart disease and therefore diagnostic coronary angiography was requested for the next day.
Diagnostic coronary angiography next day revealed 90% large proximal 1st diagonal disease. There were additional 30% plaques in various coronaries. He was not advised for stenting was told to continue ‘optimal medical therapy’ and have follow-up with me.
He came back to see me a few days later with similar original symptoms with highly anxious look and being upset with the same symptoms. He felt frustrated and unable to carry out any physical activities. I reviewed his coronary angiography findings with him. I was equally concerned after seeing 90% large proximal 1st diagonal disease and being sent home without any intervention. Keeping his symptoms and now having coronary anatomy report with me, I sent him back straight to another catheterization lab the very same day for a second opinion and likely stenting. His severe diagonal stenosis was stented and discharged home next day on optimal medical therapy.
He came back to see me a week later and this time, he was all smiles!
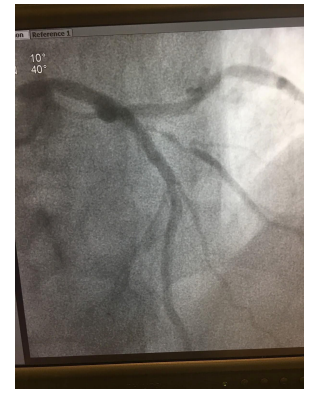
Figure 1: Coronary angiography with 95% severe Diagonal stenosis.
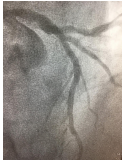
Figure 2: Same Diagonal disease after stenting.
PATIENT #2
A 54-year old man with history of diabetes, hypertension, GERD, adenocarcinoma of his left lung with metastasis to the brain status post brain surgery and intracranial bleeds in Jan 2019 now undergoing chemotherapy came to the office for cardiac evaluation with complaints of chest pressure and chest pains lasting for 12 hours and that was 2 days ago. There were no associated palpitations, jaw pains, arm pains or diaphoresis. He thought his symptoms being gastrointestinal (GI) in origin and did not seek any medical advice at the time and did not go to the emergency department.
His vitals were stable and he was chest pain free. His 12-lead EKG showed Qs inferiorly with inverted Ts in those same leads (appeared to be new).
There was no obvious wall motion abnormalities noted on his resting 2D-echocardiography in my office.
Suspicion for acute coronary syndrome with a cardiac event occurring 2 days ago was quite high and therefore I placed him on Metoprolol succinate 25 mg a day, aspirin 81 mg with food a day, rosuvastatin 10 mg a day and requested him to have routine blood tests including electrolytes, renal function. Stat troponin was ordered which came back markedly abnormal at 8.25. Therefore he was arranged to a Cardiac cath lab right away.
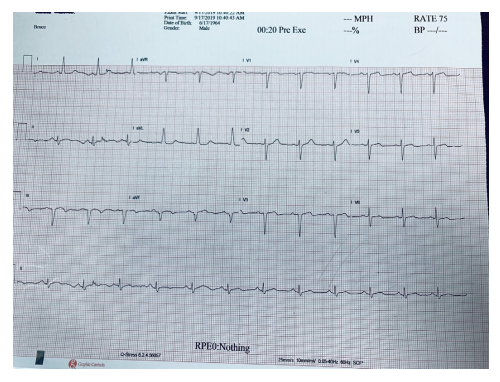
Figure 3: Normal sinus rhythm. Qs noted inferiorly in leads III and aVF and inverted Ts in the same leads.
His same day coronary angiography revealed: 2-vessel CAD with 90% mid-LAD, 70% 1st Diagonal, 100% proximal RCA disease with collaterals and LVEF of 50% with hypokinetic/akinetic inferior wall.
Based on these findings, the patient was referred to a cardiac surgeon for consultation. Surgery did not find him a suitable candidate for cardiac bypass surgery based on his history of metastatic lung CA with history of brain bleeds about 9 months prior. For the same reasons, the interventional cardiologist decided not to offer him angioplasty/stents and advised him to come back to see me to have a stress test and continue ‘the optimal medical therapy’ in the meantime!
He is a 54-year old man with a serious lung cancer presumably now much under control and he was unhappy that he was not offered coronary stenting or cardiac bypass surgery for the reason that he had intracranial bleeding 9 months before all this. He wants to live and wants to have all the right options for his heart health.
Based on his coronary anatomy report, I sent him back to another interventional cardiologist at a different hospital with the intention of coronary stenting which was performed on him and he has been doing well since then!
DISCUSSION
Cardiovascular disease (CVD) remains the leading cause of death in the US, however overall, the death rate in the US from CVD has reduced by 18.6% and from coronary heart disease by 31.8% in 10 years from 2006 to 2016. About every 40 seconds, one person in the US has a myocardial infarction (MI) and in about the same time frame, one person has a stroke as well. The annual total cost of CVD in the US in 2014-15 was estimated to be $351.2 billion [2].
Therefore based on these statistical data, we need to do everything possible to decrease the morbidity and mortality from CVD, improve the quality of life and life span of these patients and drastically reduce the cost burden on the society.
POINTS TO PONDER
Optimal Therapy versus Optimal Medical Therapy
In Cardiology, we love to use the term Optimal Medical Therapy. This case scenario happens quite often when we send patients to the catheterization lab and they do not need or do not qualify for stenting and in that case, an interventional cardiologist will send the report back stating: Optimal Medical Therapy to continue! In case of coronary artery disease, that simply means to continue a statin, a beta-blocker, an angiotensin converting enzyme inhibitor/angiotensin receptor blocker (ACEI/ARB), aspirin or clopidogrel, anti-hypertensive and/or anti-diabetic Rx as the case might be. Of course, many of these patients might not qualify for these medications: some might have lower resting heart rate and unable to take a beta-blocker; some might have tried statin and quite concerned with myalgia that they had developed before. Many might have significant renal issues and may be unable to take an ACEI/ARB; some might have had bleeding in the recent past and hesitant to try aspirin and/or Clopidogrel.
Therefore many times, this concept of Optimal Medical Therapy to continue mostly ends up being Suboptimal!
Moreover, we almost never undertake coronary stenting and not continue all these medications noted above. That means most of the time, patients get stenting when indicated along with optimal medical therapy as well. Therefore I would prefer the term Optimal Therapy as opposed to Optimal Medical Therapy.
Stenting of Smaller Branches of the Coronary Artery
In Patient #1, the 1st diagonal branch was the main culprit lesion causing his symptoms of exertional angina. I fully understand that the lesion was not in one of the major coronary arteries, however it was significantly stenosed enough that it required serious consideration for stenting right away. I also understand that the image posted here might not be the optimal way to look at the lesion, however, as much as one can see, it looks quite ‘unstable’ and leaving it to ‘optimal medical therapy’ might not have been the best option! Paying attention to the patient’s history when it comes to chest pains, angina and ischemia is of utmost value. He clearly gave history of exertional angina for a month before coming to see me. I was quite convinced of his symptoms that I placed him on certain medications right away. I was concerned enough to send him to the cath lab the very next day even though his treadmill stress test did not show any ischemic ST/T changes. All these historical clues should have been noted by the interventional cardiologist before him deciding to try ‘Optimal Medical Therapy’ and not attempt to place a stent in his Diagonal artery!
Appropriateness of Treatment
Over the last so many years the treatment of coronary artery disease/acute/chronic coronary syndrome has been so well and so extensively studied and numerous guidelines from American and European associations keep coming out from time to time. There is no dearth of knowledge, experience or training as to how to take care of these patients. We are always reminded of Hippocratic oath of ‘Do No Harm’, however, how about making sure that our patients get the Appropriate Treatment and are not being neglected and not being harmed by not getting Optimal Therapy!
Like in Patient #2, just because he has advanced lung cancer and because he has had intracranial bleeding 9 months ago, does not mean that his current treatment approach should by any means be compromised!
The reason I say that I think asking for cardiac surgery consult for cardiac bypass in this case was somewhat much less indicated based on the guidelines. The interventional cardiologist should have offered him coronary stenting for at least for his LAD artery (left anterior descending) which appeared to be the culprit lesion. Of course the risk of bleeding is there given his history of intracranial bleeding, however that was 9 month ago and he has been stable since.
Moreover, any patient that undergoes coronary stenting gets dual anti-platelet agents for sometime and we always tell the patients that they are likely to bleed on these medications. Therefore I was quite baffled to see the patient coming back to see me that an interventional cardiologist and a cardiac surgeon at a reputed University setting offered nothing but the ‘Optimal Medical Therapy’ to continue! In addition, this also brings up the interesting historical perspective for discussion: if they were so much against stenting or cardiac bypass surgery based on his history of intracranial bleeding 9 month prior, it appears imperative that the patient should not have even been offered to undergo coronary angiography in the first place!
Private Practice versus Institutional/Corporate Medicine:
A. “Consolidation of healthcare providers results in a well-documented record of harm to the patients with price increases with 20-40% after consolidation”: America’s health insurance plans [3].
B. “Physician-hospital consolidation has not led to improved quality or reduced costs… and is often motivated by a desire to expand bargaining power by reducing competition.”: Robert Wood Johnson Foundation [4].
Why Private Practitioners Are Still the Best Choice for Patients:
A private practice is your best bet for receiving the highest quality of care at the lowest cost. (US News October 2018; Dr Nicholas Grosso) [5].
(Forbes, September 2016) [6].
SUMMARY
We are always encouraged to follow the various guidelines to practice medicine in general, however, we are also reminded to personalize those guidelines to individual patients. Likewise in the same vein of arguments, I would encourage to keep the US Health Care the option of Private Practice of Medicine alive and well. In huge corporate world of medicine and larger institutions of health care, while fostering and strictly following the national guidelines, at times we tend to forget that we are dealing with individuals. Patients are recognized as individuals more often in a private medical practice setting than otherwise. Granted that private practice physicians might have financial incentive to take care of people and their medical problems, but then where do we want to spend our money the most: on a house, a car, the road construction, business building or improving and taking care of human lives? Everything can be bought, sold and replaced but not your life!
In both cases, patients were initially sent to a University setting and I assume they followed the guidelines (or maybe not). Because the symptoms persisted, the optimal treatment was offered in each case, both were sent to another institution: to a private practitioner/interventional cardiologist and he took care of both patients quite well. He might have had a financial incentive to do things, however, it was clearly indicated to relieve patients symptoms (Case # 1) and protect the heart (Case #2). It is logically possible that he did his ‘best’ to take care of these patients so that more patients would be referred to him in the future! Well, we want that ‘bestness’ of all the docs to survive and persist and therefore I would insist on public and politicians to not only make sure that Private Practice remains an option but prevails as a dominant, existing and alternative option in the modern world of medicine where Dollar is taking over the Disease and Money is more important than man!
REFERENCES
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al. (2010) Heart disease and stroke statistics-2010 update: a report from the American Heart Association. Circulation 121(7): e46-e215.
- Benjamin EJ, Muntner P, Alonso A, Marcio S Bittencourt, Clifton W Callaway, April P Carson, et al. (2019) Heart disease and stroke statistics-2019 update: A report from the American Heart Association. Circulation 139(10): e56-e528.
- America’s Health Insurance Plans [Internet].
- Robert Wood Johnson Foundation [Internet].
- US News October 2018; Dr Nicholas Grosso [Internet].
- Forbes, September 2016 [Internet].
Copyright: Mishra JP, et al. ©2019. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation: Mishra JP (2019). A Tale of Two Treatments. Cardiac 1(1): 5.